

Acoustic Neuroma
( Vestibular Schwannoma ) Acoustic neuroma is a benign tumor that grows in the internal auditory canal and affects the hearing, facial, and balance nerves.Overview of Acoustic Neuroma
What is an acoustic neuroma?
An acoustic neuroma is a benign tumor that can affect the balance and hearing nerves behind the inner ear. Tumors are classified as benign or malignant based upon their growth characteristics. Benign tumors generally grow slowly and do not spread throughout the body. When they grow, they usually invade or push adjacent structures aside. Unlike benign tumors, malignant tumors like breast cancer, colon cancer, lung cancer, and prostate cancer generally grow faster and can spread to other regions of the body.
Where are these acoustic neuromas?
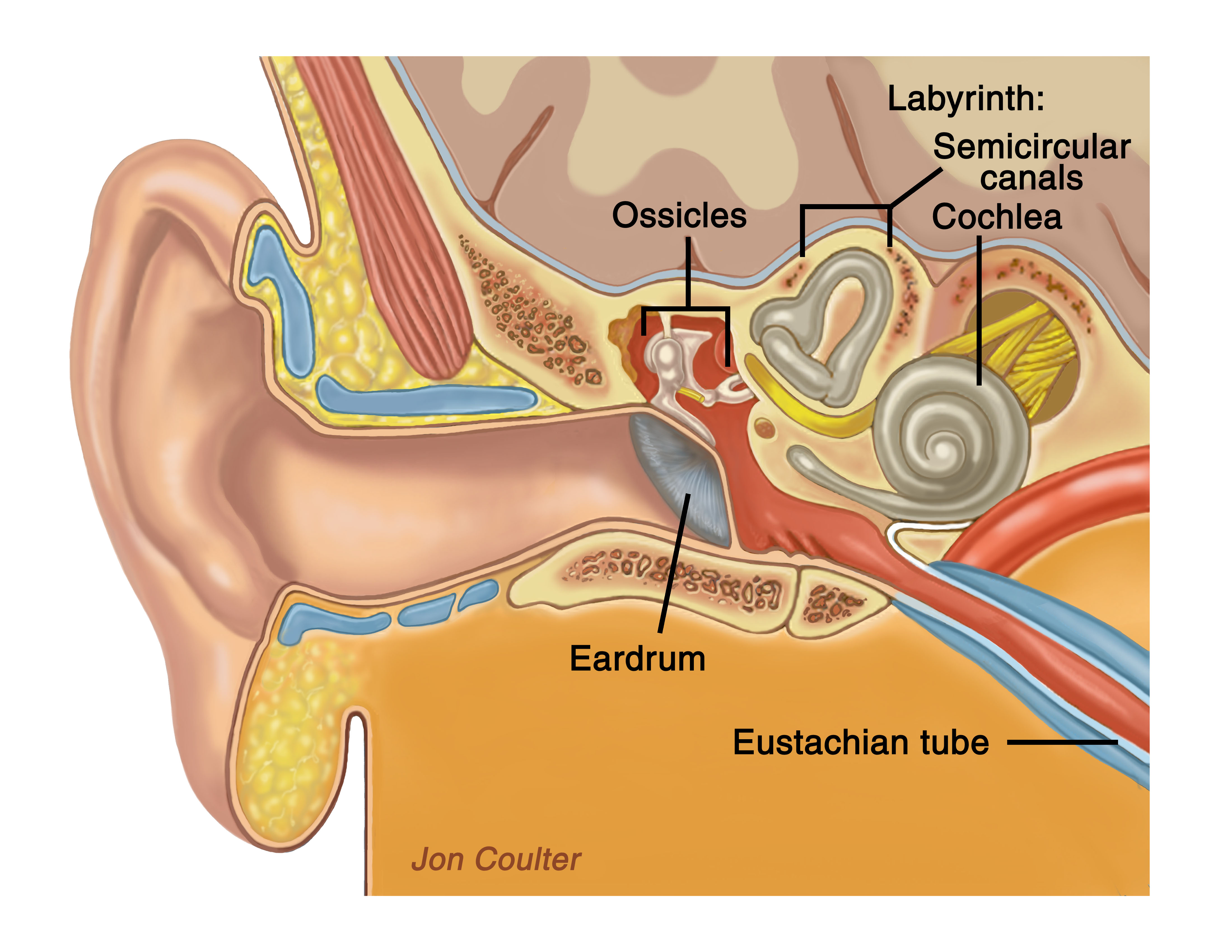
The temporal bone anatomy is shown, including the ear canal, ear drum, middle ear, and inner ear.
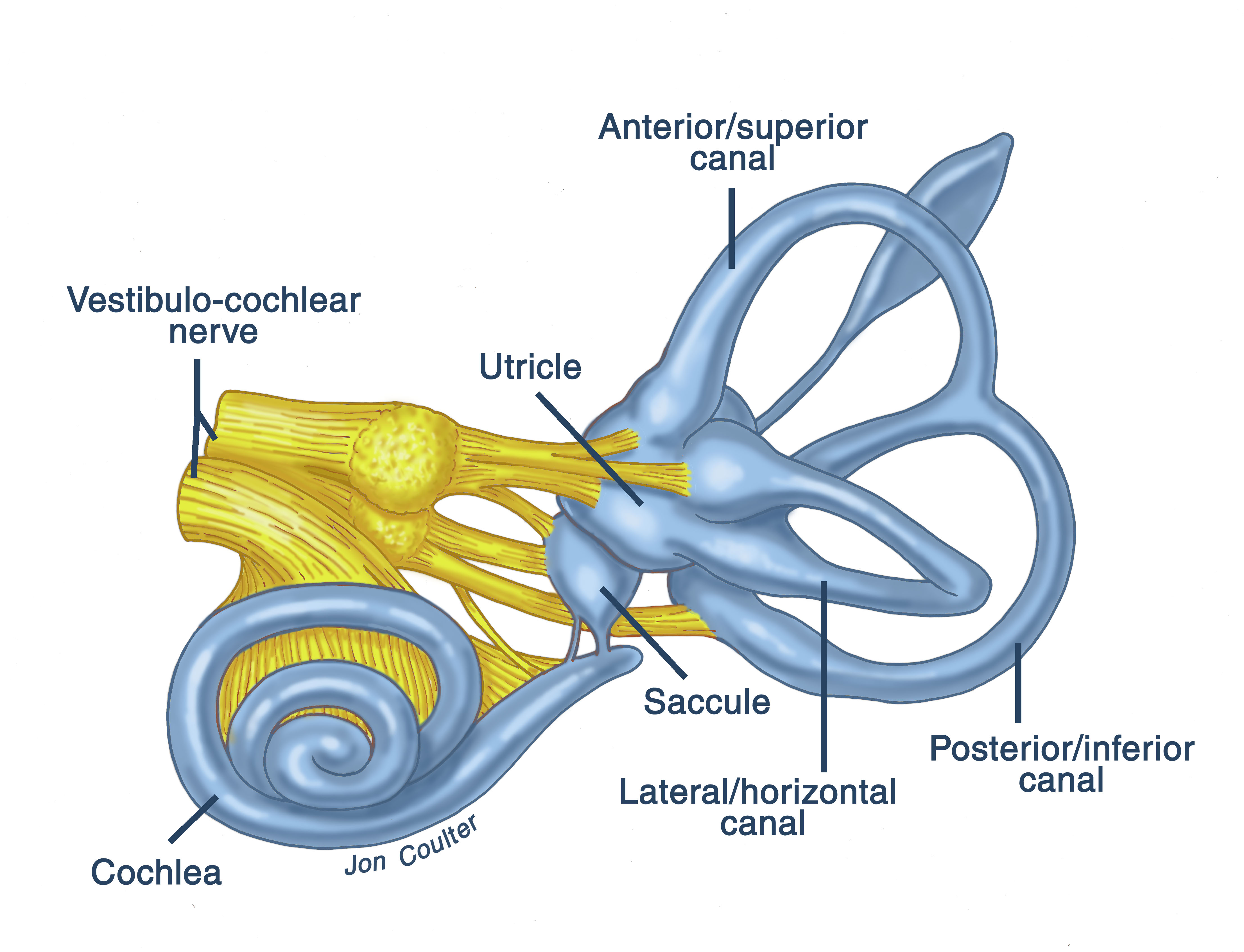
The inner ear anatomy is shown, including the semicircular canals, the cochlea, and nerves.
A brief description of the anatomy of this region is described. Sound entering the ear canal causes vibrations of the tympanic membrane (eardrum). The eardrum is attached to one of three ossicles (bones) found in the middle ear called the malleus. The malleus bone transmits the mechanical vibrations to another ossicle, the incus, which in turn transmits the vibrations to the smallest of the three ossicles, the stapes. The stapes bone vibrates and transmits the mechanical energy to the inner ear. The inner ear is made of a bony labyrinth filled with fluid and membranes. As the stapes vibrates, the fluid in the inner ear is set into motion. The cilia on the ends of hair cells within the inner ear are bent and an electrical signal is generated. This travels along the cochlear (hearing) nerve and then back to the brain. The inner ear is composed of the cochlea, which is responsible for hearing, and the semicircular canals that convey balance information concerning angular acceleration of the head back to the brain. Two other organs, the saccule and the utricle, found in the inner ear detect linear acceleration of the head.
The internal auditory canal contains three different types of nerves: the cochlear (hearing), vestibular (balance) and facial nerve. The facial nerve is responsible for contraction of the facial muscles, thus allowing motion of the face on that side. This is the nerve that is responsible for our ability to raise our eyebrows, close our eyes, flare our nostrils, and raise the corner of the mouth on that side. It is also responsible for conducting information regarding taste from the front 2/3 of the tongue and also tear production from the lacrimal glands.
The superior and inferior vestibular nerves (or upper and lower balance nerves) transmit linear and angular acceleration data to the central nervous system. Peripherally, (i.e. closer to the inner ear) the superior and inferior vestibular nerves are coated by a layer of Schwann cells which produce a substance called myelin. Myelin insulates the nerves and allows efficient conduction of nerve impulses. Centrally, (i.e. closer to the brainstem) these nerves are coated by a layer of cells called oligodendroglia, which have the same function as Schwann cells. The junction where the Schwann cells meet the oligidendroglia cells is termed the Obersteiner-Redlich zone. Acoustic neuromas arise from Schwann cells located near the Obersteiner-Redlich zone and are more appropriately termed vestibular schwannomas.
How common are these tumors?
According to a Danish study, the frequency with which these tumors occur is 10-13 cases per million general population. Accurate data on prevalence and incidence in the United States is not available.
What are the symptoms that indicate the possibility of a tumor?
Hearing loss or tinnitus (ringing in the ears), especially if greater in one ear as compared to the other, may be the first signs of the presence of a tumor. Mild disequilibrium can occur as more of the vestibular nerve is destroyed. Numbness or tingling in the face may indicate that a larger tumor is pressing on the trigeminal nerve, the nerve that transmits facial sensation (not motion). As the tumor gets larger, it can press on the cerebellum and pons to cause severe disequilibrium. With even larger tumors, spinal fluid pathways within the brain can become obstructed and can cause a condition called hydrocephalus. Nausea, vomiting, and headache are common with this condition. Progressive growth can lead to a comatose state and eventual death.
What is the growth rate of these tumors?
These tumors vary in regards to growth rate. The growth rate can vary from 0.1 mm to 10.0 mm per year. Growth does not necessarily follow a linear curve. Some tumors may remain relatively stable for some years followed by rapid growth thereafter. Growth remains unpredictable. There is evidence to show that tumors having a cystic appearance on an MRI scan can grow at a much more rapid rate of 20 to 35 mm per year. I believe these tumors require earlier intervention.
About Dr. Prasad

Dr. Sanjay Prasad MD FACS is a board certified physician and surgeon with over twenty years of sub-specialty experience in Otology, Neurotology, advanced head and neck oncologic surgery, and cranial base surgery. He is chief surgeon and founder of the private practice, Metropolitan NeuroEar Group, located in the metropolitan Washington D.C. area.
Find us on Facebook
Follow us on Twitter
- AcousticTumor tweeted Visit our brand new educational website, http://t.co/rVFYMnnJ, for more information about acoustic neuromas and their treatment!October 27, 2011 at 11:21am
- AcousticTumor tweeted Our website has launched! http://t.co/s3Ft7Rn3October 27, 2011 at 11:21am
- AcousticTumor tweeted Have you been diagnosed with an acoustic neuroma? Need information on what it is? Want access to others with the same condition? Follow us!January 07, 2011 at 12:48pm